
k-t bFFE Real-Time M2D
Instructions for acquiring multi-2D k-t bFFE real-time MRI
Summary:
- repeat prescans before every kt8i0bffe_m2d scan
- start delayed reconstruction once next kt8i0bffe_m2d scan is running
- prescribe scan planes and FOVs carefully to avoid fold-over in phase encode direction
- set FOV in read-out direction to multiple of 16, i.e., 272, 288, 304, 320, 336, 352, 368, 384, 400 mm
updated 19 Sept 2017
Sequences
examcard - Hospital > Foetal > FetalCMR_RealTime_AddOn_20170917
kt8i0bffe_m2d - k-t sampled multi-2d real-time (~17s per slice)
btfe_m2d_ref - bTFE scout (<10s)
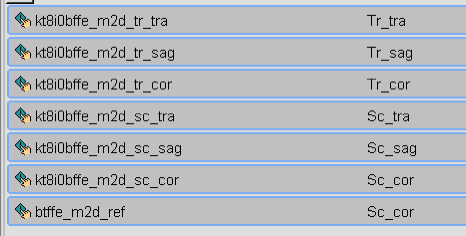
suggested planes
tr_tra - transverse to fetal trunk
tr_sag - sagittal to fetal trunk
tr_cor - coronal to fetal trunk
sc_tra - scanner transverse (i.e., x-y)
sc_sag - scanner sagittal (i.e., y-z)
sc_cor - scanner coronal (i.e., x-z)
Before Scanning
- enable PIH1 patch
- append sequences to current examcard
During Scan
Coverage & Planning
In-Plane
Fold-over in the phase encode direction results in artefact reconstructed images.
Planning
The scanner canonical orientations can usually be planned against sequences that have already been acquired during the exam, e.g., chest_btfe_tra/sag/cor, but in some cases, and for oblique planes, additional steps may be helpful.
- generate orientations using volume viewer on a recent scan (e.g., btfe_uterus_sag), and then prescribe orientation using three-point plan to the derived images, or
- run the btfe_m2d scout prior to the real-time scan and adjust the scan plane angulation and in-plane orientation accordingly
Field-of-View
The FOV can be adjusted to avoid fold over in the phase-encode direction while achieving the best temporal resolution possible.
For the scan parameters in the examcard,
* repetition time (TR) is 3.8 ms
* phase-encode resolution (dy) is 2 mm
* FOV in phase-encode direction (FOVy) is 304 mm
* k-t acceleration factor (R) is 8
* number of acquired phase-encode lines (Ny) is 152
- Ny = FOVy / dy, or
- Ny = 304 mm / 2mm = 152 lines
* temporal resolution (dt) is 72 ms
- dt = TR * n_y / R, or
- dt = 3.8 ms * 152 / 8 = 72 ms
Phase-Encode Direction
The FOV in the phase-encode direction should be as small as possible in order to optimise temporal resolution.
When changing the FOV, it is ideal to use multiples of sixteen, i.e., 272, 288, 304, 320, 336, 352, 368, 384, 400 mm.
Readout Direction
It is best to leave the field of view in the readout direction as it is.
Reduction of the field of view in the readout direction will not have a significant impact on temporal resolution but will have a relatively larger detrimental impact on SNR.
Through-Plane
The number of slices can be increased to cover fetal heart.
It is better, for volume reconstruction purposes, to collect more m2d stacks with coverage of the central mass of the heart than fewer m2d stacks with more slices covering extra-cardiac anatomy.
Bug 'scan requires too many prescans'
This is a bug in the system software beyond our control.
It occurs unpredictably when the current scan requires a SENSE reference or coil survey prescan, resulting in wasted exam time and may also corrupt sequence parameters.
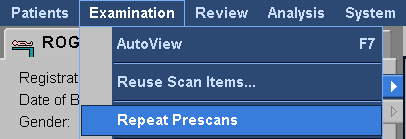
To avoid the bug, it is safest to force the system to acquire new prescans before running any real-time sequence:
* Examination > Repeat Prescans
* this can be done while the previous scan is running
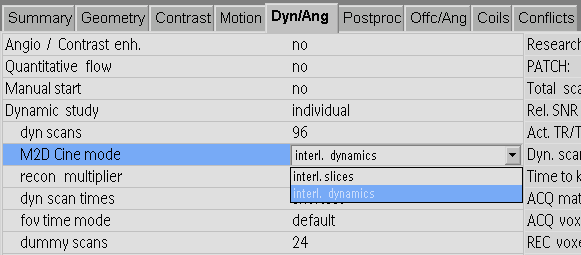
If the bug does occur: * check that Dyn/Ang > M2D Cine mode = 'interl. dynamics', and -not- 'interl. slices' * repeat the scan after the 'Repeat Prescans' command
Scan Duration
Scan duration will be twice the time reported on the scanner console.
This is the case for any sequence that uses k-t sampling with separate training data.
After Scanning
Delayed Reconstruction
Image reconstruction can tie up system resources and the system will wait to start the next scan.
To avoid this downtime, start delayed reconstructions just after the current scan starts running.
Archiving
- send .raw/.lab/.sin/.log to pnraw using GyroTools' PackNGo
- if possible, also save the examcard and protocol text files